Neurofeedback is grounded in decades of neuroscience research. Studies show benefits for ADHD, anxiety, depression, PTSD, insomnia, and cognitive optimization.
Historical Context
Neurofeedback, also known as electroencephalographic (EEG) biofeedback, emerged in the 1960s from foundational research on operant conditioning of brainwaves. Early work by Barry Sterman and colleagues demonstrated that animals could learn to increase sensorimotor rhythm (SMR) frequencies, leading to human applications for seizure reduction. Over subsequent decades, neurofeedback evolved to encompass diverse EEG frequency bands, quantitative EEG (qEEG) mapping, and advanced modalities such as slow cortical potentials (SCP), low-resolution electromagnetic tomography (LORETA), and functional near-infrared spectroscopy (fNIRS). By the early 2000s, clinical protocols were systematized for attention-deficit/hyperactivity disorder (ADHD), anxiety, mood disorders, and trauma-related dysregulation.
Mechanisms of Action
Neurofeedback operates through operant conditioning, a process by which the brain learns to modify its own electrical activity in response to real-time feedback. EEG sensors measure cortical oscillations (brainwave frequencies such as alpha, beta, theta, delta, and gamma). The signal is processed by software that translates these patterns into visual, auditory, or tactile feedback—typically a moving image or tone. When desired frequency patterns increase (e.g., higher SMR or reduced theta/beta ratio), the client receives positive reinforcement (e.g., a game moves smoothly, music continues). Over repeated sessions, the brain gradually stabilizes toward the trained target patterns, reflecting improved self-regulation.
Typical Process
Assessment and Baseline Mapping
The process begins with an intake evaluation and a quantitative EEG (qEEG) or brain map, which identifies atypical amplitude or coherence patterns relative to normative databases. This guides protocol selection (e.g., training alpha up, beta down).Sensor Placement and Calibration
Sensors (non-invasive scalp electrodes) are placed according to the 10–20 system, commonly over frontal, central, or parietal sites depending on goals (e.g., C3/C4 for SMR training).Training Phase
The client engages in feedback tasks lasting 20–40 minutes. Feedback may appear as a video game, bar graph, or animation. The system rewards EEG states consistent with the target (e.g., increased focus or relaxation patterns) and inhibits non-target frequencies.Review and Adjustment
The clinician monitors session metrics—reward ratios, threshold attainment, and artifact control (e.g., eye blinks, muscle tension)—and adjusts parameters to maintain optimal challenge.Integration and Reflection
Clients often discuss subjective experiences (e.g., changes in mood, focus, or sleep) post-session. Protocols are adapted progressively based on both EEG and self-report trends.
Duration and Number of Sessions
The number of neurofeedback sessions varies by condition and individual neuroplasticity. Evidence-based ranges are as follows:
ADHD and attention regulation: 30–50 sessions
Anxiety and stress regulation: 20–40 sessions
Sleep disturbances: 20–30 sessions
Trauma-related dysregulation (e.g., PTSD): 40–60 sessions
Peak performance training: 10–20 sessions
Sessions typically occur 1–3 times per week, with cumulative effects becoming apparent after approximately 10–15 sessions. Consolidation and maintenance may require periodic booster sessions after the main course of training.
Physiological and Psychological Effects
Neurofeedback facilitates self-regulation of central nervous system activity, improving cortical stability, arousal modulation, and cognitive flexibility. Consistent training has been associated with reduced impulsivity, enhanced executive function, improved emotional control, and normalization of sleep–wake rhythms. Because learning is endogenous and gradual, changes are typically durable, reflecting long-term neural adaptation rather than transient state changes.
We work with brain networks that regulate attention, emotion, and resilience. QEEG helps identify disruptions in networks like the default mode network, salience network, and attention networks, guiding more precise interventions.
Brainwaves
Depending on where and when they show up, brainwaves can reveal a lot about a person.
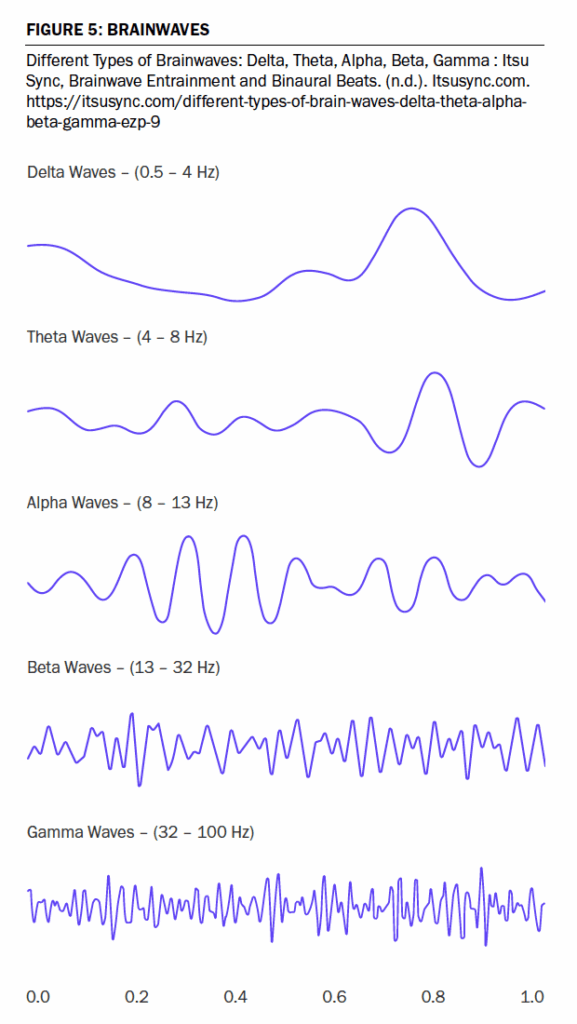
Delta: Deep sleep, memory consolidation, a carrier rhythm. In abnormal cases, when found in certain areas while awake, delta can be an indicator of white matter damage (axonal sheering) due to head injury.
Theta: Focus, memory, creativity, intuition, emotional clarity, and insight. Children spend most of their time in theta. Persistent theta frontally can be an indicator of attention issues.
Alpha: Relaxed but alert, the brain’s idling rhythm generated by the thalamus, seen during transitions between internal and external attentional modes. Peak alpha frequency seen in the back of the head with eyes closed is considered an index of individual differences in cognitive processing speed, working memory capacity, and general arousal levels. Slower PAF may be associated with reduced information processing speed; faster PAF may correspond to more efficient neural communication.
Beta: Active concentration, complex problem-solving, rumination or potentially anxiety.
Gamma: Learning new concepts, integration of information, innovation, clarity, and even deep states of meditation. However, when persistent and global gamma can be pathological.
Ethics & Data Use
In alignment with the IQCB Code of Ethics, we only use de-identified client data for research purposes, and only with explicit consent.